A tale of two health systems...
My experience of the health system in the US has been mixed. I have had a couple of medical issues over the last 18 months that have required timely attention. The doctors, nurses, facilities, and administrators have all been excellent. The doctors have been able to order procedures and tests when they want, and I have had minimal wait times. For example, in December my doctor decided I should meet with a surgeon. I got an appointment with the surgeon in early January and then we scheduled the surgery for early February, not because he couldn't fit me in sooner but because he wanted a slight delay while certain medications left my system.
On the other hand, understanding and dealing with the health insurance has been confusing and dispiriting. Mr Husband's TechGiant company pays for extremely comprehensive private health insurance. We have a relatively high deductible (we pay the first $4,000 of our medical expenses each year) but after that, everything is 'free' (or paid for, so feels free) provided the insurance company thinks the expense is justified.
Here is where it becomes complicated. Last summer my doctor ordered a routine blood test to check the if a drug level was correct. A few weeks later we received a bill for $2,500 from the lab that processed the test. The bill said the health insurance company had refused to pay, but also said that we should not pay anything yet; the lab would appeal the decision on my behalf. So began a six month dance between the lab and health insurance that culminated in a letter from the health insurance company saying that, after reviewing the published studies on this blood test, "there is not enough information in the medical literature to show that is safe, effective, and medically necessary for your condition." The confusing and apparently contradictory part of the story was that based on the blood test, my doctor had doubled the dose of the medication, and the insurance company had approved the cost of new dose.
I asked my doctor what to do next, and he said to get back to the lab and they would likely soak up the cost (still working on that!). He also ranted for about ten minutes about the health insurance system in the US. I talked with a few Americans about what to do and their attitude was 'just pay, don't question the health insurance company, it's too risky'. (Admittedly this advice was from a woman who owns multiple polo ponies!) So even though we have excellent private coverage, we still have considerable out-of-pocket costs. This is not an option for most of America, leading to people being under-insured or having no insurance.
An additional flaw is that there is no actual healthcare 'system'. To date our family has accessed six different practices, none of whom talk to each other or share records without paperwork, all of whom have multiple employees whose specific job is to coordinate with health insurance companies. The mind boggles at the inflated costs due to duplication and bureaucracy.
I have experienced both the National Health Service in the UK and the province-funded system in Canada. I have been treated well in both and am an ardent believer in publicly funded health systems. However, I am conflicted. My treatment and outcomes over the past 18 months have undoubtedly been better here in the US. If I had been asked seven weeks ago (around the time of my surgery) to evaluate the US healthcare system I would probably have would have overlooked my two gripes above - expense/uncertainty of health insurance and lack of coordinated system - and said it was excellent.
That was my view of the US health system then, just seven weeks ago.
Now, through the lens of the pandemic, I see a different story. These two flaws alone reveal severe inadequacies.
While President Obama's Affordable Care Act of 2010 overhauled and greatly expanded the Medicaid and Medicare programs to help cover people over 65 and low-income individuals, the Center for Disease Control and Prevention (CDC) reports that 11% of Americans are still completely uninsured. 65% have private health insurance and 25% have public health insurance. A key concern in the early days of the virus spreading in the US was that people would both continue to work while sick and not seek medical help due to the expense. Furthermore, the lack of an efficient, coordinated nationwide or even statewide system contributed to the lack of testing across the country. In the early days of the outbreak, all tests had to be run through the CDC, with results taking two weeks or more. The FDA was slow to approve other labs to run tests, and eventually states took matters into their own hands and authorized local labs to provide testing.
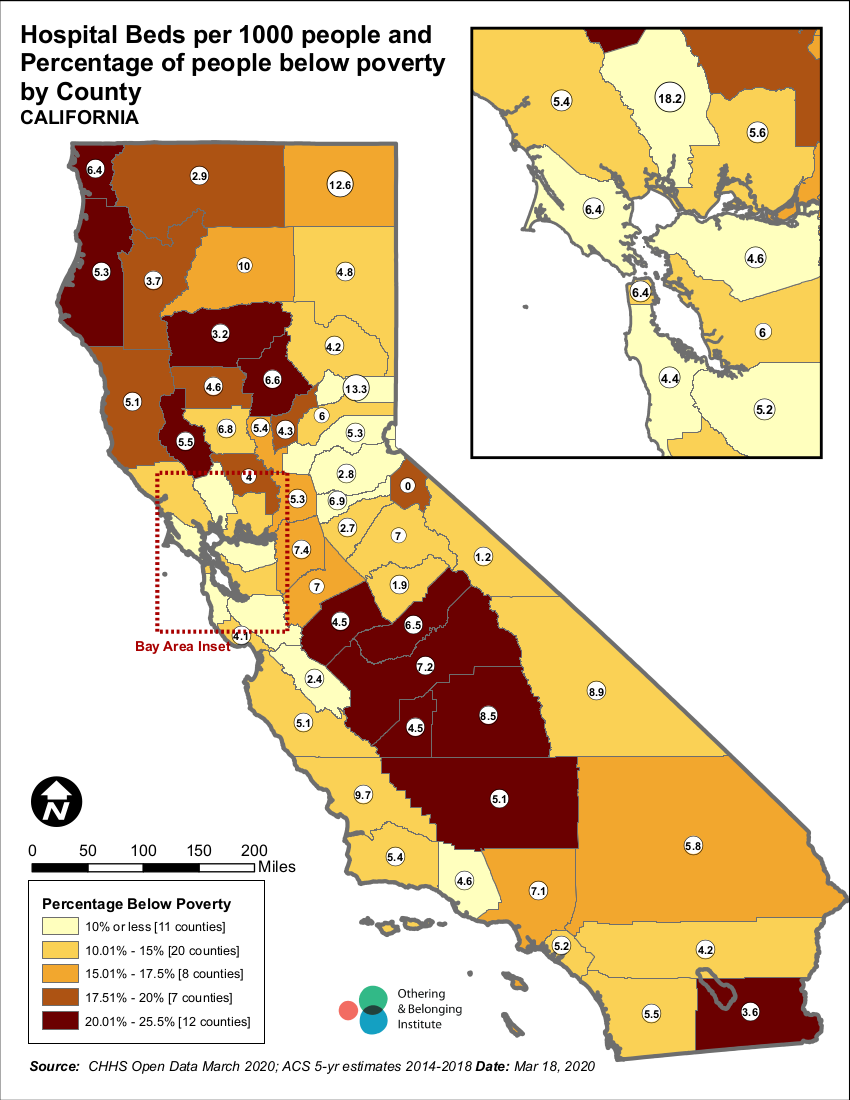
Finally, a friend in Canada just sent me some interesting maps showing number of beds per capita in California. The Othering and Belonging Institute at UC Berkeley has launched a mapping project to help identify populations and regions particularly vulnerable to COVID-19. The maps show that the number of hospital beds per 1000 people by county ranges from 1.9 to 13. And while regions with low numbers of beds do correlate with poverty and in particular non-white poverty, the high-income regions do not have particularly high numbers of beds per 1000 people.
Based on a sample size of one, I wonder if my recent experience offers some insight. I was in the Mills-Peninsula Medical Center, a state-of-the-art 241-bed hospital opened in 2011 that is one of 23 hospitals that serves the mid-peninsula and south bay (San Mateo and Santa Clara counties with 4.4 and 5.2 beds per 1000 people respectively). Every room in Mills-Peninsula is private and came with room service! It felt pretty wonderful to be there but it wasn't designed to respond to a public health crisis. I wonder how many of the hospitals in this region are similar?
I found this OECD data that shows that our local numbers of beds are slightly higher than the national number. The graph below compares countries. I've highlighted some countries of interest. Canada, the UK, the US, Spain and Italy all have between 2-3.5 hospital beds per 1000 people. China has 4, France 6. Korea and Japan are just over 12.
Another strange phenomenon I encountered was that the night and weekend shifts were populated by 'travel nurses'. These were nurses who take temporary contracts around the country as needed. I met nurses who had homes in Texas, Ohio, and Colorado. Some were on short contracts (matters of weeks) others were here for multi-year contracts. I wonder what is happening now with the lockdowns? On the one hand, great to have this shifting, flexible workforce. But not when travel itself can spread disease and increase the risk of catching the virus.
Today's news is that the numbers of hospitalized patients in New York has jumped by 40% in one day. The US now has the most number of COVID-19 cases.
This quote has been over-used in making comparisons to many modern situations, but Dicken's description of the French Revolution has never seemed more apt in describing the America of today.
On the other hand, understanding and dealing with the health insurance has been confusing and dispiriting. Mr Husband's TechGiant company pays for extremely comprehensive private health insurance. We have a relatively high deductible (we pay the first $4,000 of our medical expenses each year) but after that, everything is 'free' (or paid for, so feels free) provided the insurance company thinks the expense is justified.
Here is where it becomes complicated. Last summer my doctor ordered a routine blood test to check the if a drug level was correct. A few weeks later we received a bill for $2,500 from the lab that processed the test. The bill said the health insurance company had refused to pay, but also said that we should not pay anything yet; the lab would appeal the decision on my behalf. So began a six month dance between the lab and health insurance that culminated in a letter from the health insurance company saying that, after reviewing the published studies on this blood test, "there is not enough information in the medical literature to show that is safe, effective, and medically necessary for your condition." The confusing and apparently contradictory part of the story was that based on the blood test, my doctor had doubled the dose of the medication, and the insurance company had approved the cost of new dose.
I asked my doctor what to do next, and he said to get back to the lab and they would likely soak up the cost (still working on that!). He also ranted for about ten minutes about the health insurance system in the US. I talked with a few Americans about what to do and their attitude was 'just pay, don't question the health insurance company, it's too risky'. (Admittedly this advice was from a woman who owns multiple polo ponies!) So even though we have excellent private coverage, we still have considerable out-of-pocket costs. This is not an option for most of America, leading to people being under-insured or having no insurance.
An additional flaw is that there is no actual healthcare 'system'. To date our family has accessed six different practices, none of whom talk to each other or share records without paperwork, all of whom have multiple employees whose specific job is to coordinate with health insurance companies. The mind boggles at the inflated costs due to duplication and bureaucracy.
I have experienced both the National Health Service in the UK and the province-funded system in Canada. I have been treated well in both and am an ardent believer in publicly funded health systems. However, I am conflicted. My treatment and outcomes over the past 18 months have undoubtedly been better here in the US. If I had been asked seven weeks ago (around the time of my surgery) to evaluate the US healthcare system I would probably have would have overlooked my two gripes above - expense/uncertainty of health insurance and lack of coordinated system - and said it was excellent.
That was my view of the US health system then, just seven weeks ago.
Now, through the lens of the pandemic, I see a different story. These two flaws alone reveal severe inadequacies.
While President Obama's Affordable Care Act of 2010 overhauled and greatly expanded the Medicaid and Medicare programs to help cover people over 65 and low-income individuals, the Center for Disease Control and Prevention (CDC) reports that 11% of Americans are still completely uninsured. 65% have private health insurance and 25% have public health insurance. A key concern in the early days of the virus spreading in the US was that people would both continue to work while sick and not seek medical help due to the expense. Furthermore, the lack of an efficient, coordinated nationwide or even statewide system contributed to the lack of testing across the country. In the early days of the outbreak, all tests had to be run through the CDC, with results taking two weeks or more. The FDA was slow to approve other labs to run tests, and eventually states took matters into their own hands and authorized local labs to provide testing.
 |
| See https://belonging.berkeley.edu/sites/default/files/hospital_beds_poverty.png |
{kind=link}
Finally, a friend in Canada just sent me some interesting maps showing number of beds per capita in California. The Othering and Belonging Institute at UC Berkeley has launched a mapping project to help identify populations and regions particularly vulnerable to COVID-19. The maps show that the number of hospital beds per 1000 people by county ranges from 1.9 to 13. And while regions with low numbers of beds do correlate with poverty and in particular non-white poverty, the high-income regions do not have particularly high numbers of beds per 1000 people.
Based on a sample size of one, I wonder if my recent experience offers some insight. I was in the Mills-Peninsula Medical Center, a state-of-the-art 241-bed hospital opened in 2011 that is one of 23 hospitals that serves the mid-peninsula and south bay (San Mateo and Santa Clara counties with 4.4 and 5.2 beds per 1000 people respectively). Every room in Mills-Peninsula is private and came with room service! It felt pretty wonderful to be there but it wasn't designed to respond to a public health crisis. I wonder how many of the hospitals in this region are similar?
I found this OECD data that shows that our local numbers of beds are slightly higher than the national number. The graph below compares countries. I've highlighted some countries of interest. Canada, the UK, the US, Spain and Italy all have between 2-3.5 hospital beds per 1000 people. China has 4, France 6. Korea and Japan are just over 12.
 |
| See original at https://data.oecd.org/healtheqt/hospital-beds.htm |
Another strange phenomenon I encountered was that the night and weekend shifts were populated by 'travel nurses'. These were nurses who take temporary contracts around the country as needed. I met nurses who had homes in Texas, Ohio, and Colorado. Some were on short contracts (matters of weeks) others were here for multi-year contracts. I wonder what is happening now with the lockdowns? On the one hand, great to have this shifting, flexible workforce. But not when travel itself can spread disease and increase the risk of catching the virus.
Today's news is that the numbers of hospitalized patients in New York has jumped by 40% in one day. The US now has the most number of COVID-19 cases.
This quote has been over-used in making comparisons to many modern situations, but Dicken's description of the French Revolution has never seemed more apt in describing the America of today.
“It was the best of times, it was the worst of times, it was the age of wisdom, it was the age of foolishness, it was the epoch of belief, it was the epoch of incredulity, it was the season of light, it was the season of darkness, it was the spring of hope, it was the winter of despair.”A Tale of Two Cities, Charles Dickens, 1859
Comments
Post a Comment